Dr. Koutures Quoted in: Girls More Prone to Sports Injuries- Here's Why

Please Check Our New Brand and Website: www.ActiveKidMD.com
Comprehensive blend of general pediatric and sport medicine care with an individualized approach that enhances the health and knowledge of patients and their families
ACCEPTING NEW PATIENTS- CALL 714-974-2220 FOR AN APPOINTMENT
CLICK HERE FOR DR. KOUTURES GENERAL PEDIATRICS INFORMATION
Proud physician:
USA Volleyball Mens/Womens National Teams
CS Fullerton Intercollegiate Athletics
Chapman University Dance Department
Orange Lutheran High School
Co-Author of Acclaimed Textbook
Pediatric Sports Medicine: Essentials for Office Evaluation
Orange County Physician Of Excellence, 2015 and 2016
What is going on with all these serious knee injuries in youth sports? Why do young women seem to tear their Anterior Cruciate Ligaments more than young men?
If your daughter (or son) lands with the knee caving in towards the other knee, then this article is a must read
The Anterior Cruciate Ligament (ACL) is a support ligament inside the knee that travels from the femur (thigh bone) to the tibia (shin bone), limits excessive forward motion of the tibia, and is crucial to overall knee stability.
Seemingly innocent, non-contact movements such as landing from a jump, twisting, cutting, or knee hyperextension are the most common mechanisms for ACL tears.
Studies involving several sports (basketball, volleyball, soccer) indicate that young women tear the ACL at a higher rate than young men. Several theories abound as to the reason, and a more popular thought is that abnormal landing mechanics can increase injury risk.
A preferred landing or turning occurs with the hip, kneecap and second toe lined up. Land or turn with a knee that "collapses" inside of the hip and second toe (much like the picture above) and the knee injury risk goes higher.
Tearing an ACL brings up some difficult decisions. The athlete can select sports that do not involve cutting or jumping, or if they wish to continue higher-risk activity, surgical reconstruction with 6-9 month rehabilitation periods may be needed. Without activity modification, very few young, active athletes can return to high-level sports without frequent knee pain, instability and swelling.
Does the increased chance of injury mean that young athletes should not play higher-risk sports?
Of course not.
I definitely think that the higher risk potential requires that certain precautions be taken to help protect the knees.
How can an athlete protect his/her knees?
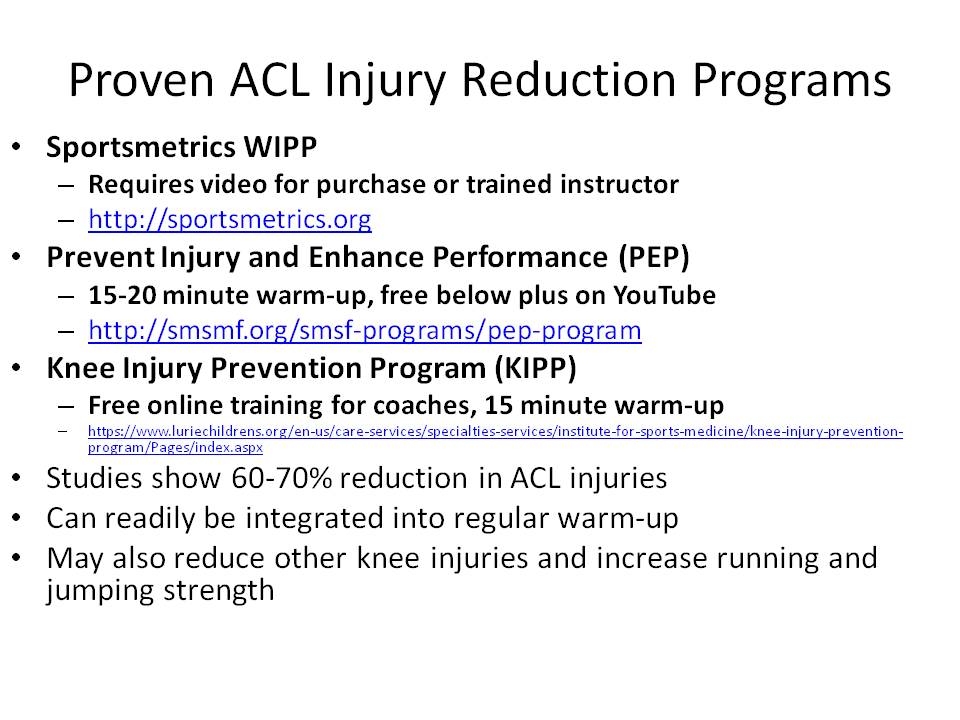
Sports-specific ACL injury reduction and knee neuromuscular training programs have been developed based on good studies that show significant reduction in ACL injuries.
Contact me for further details and specific drills/exercises particularly designed for use in weekly soccer practice warm-ups and can be applied to other jumping sports such as basketball and volleyball.
Other Knee Friendly Techniques include:
1. In youth soccer, most lower body injuries come from non-body contact and occur more in competition than training or practice sessions. While training injury incidence rates usually do not change with increased player age, match injury incidence tends to increase with age through all age groups
2. The time of the adolescent growth spurt (girls usually age 12-14 and boys usually age 13-16) seems to have an increased vulnerability for traumatic injuries. Afterwards athletes seem to be susceptible to cumulative overuse injuries.
3. Knee injuries occur in 7% to 36% of injured players and are seen more frequently in females Middle school soccer playing females have a higher rate of anterior knee pain issues than volleyball or basketball players. Any single-sport adolescent female has a higher risk of anterior knee pain issues.
4. Adolescent female soccer players suffer a roughly 3-6 times increased risk of ACL rupture compared to boys playing the same sport. Several factors have been proposed for the increased risk, such as anatomic differences, hormonal contributions with menstrual cycles, and higher-risk single-leg landing, turning, and jumping positions.
6. Ankle injuries account for 16% to 29% of injuries and are more frequent in male and older players Ankle contusions more common in younger players due to the more ground-oriented game, while in older players ankle sprain tend to occur due to the more aggressive and faster game.
9. Greater exposure to training and competition leads to a greater risk of injury due to the high intensity of the activities.
What ideas do I have to help reduce these risks?
What ideas would you add to help young soccer players reduce lower body injuries?
Below is a copy of the slide presentation:
As if tearing an Anterior Cruciate Ligament (ACL) the first time isn't wonderful enough, the risk of a similar second injury within 24 months of returning to sport is frighteningly high, according to a recent study published in the American Journal of Sports Medicine.
In the population of 78 patients (mean age 17.1 years) who underwent surgical ACL reconstruction and made a return to cutting and twisting sports:
in my opinion, this high rate of second injury, especially in the opposite knee, adds even more evidence to the already strong suggestions that improper lower extremity mechanics play a significant role in ACL tears and that neuromuscular training programs are absolutely essential for prevention especially in female participants in high risk activities such as soccer, volleyball, basketball, gymnastics and lacrosse.
Thankfully, there are several evidence-based programs readily found at no charge:
Best started as athletes reach early puberty (age 12-14), all of these programs feature stretching, strengthening, plyometric training and sport-specific agility exercise that all together take no more than 15 minutes and can easily be integrated into a regular warm-up routine that has been effectively taught to coaches both in-person and on-line.
No reasonable excuses exist for not utilizing these programs. The supporting science is solid, the programs aren't difficult to find or learn, and the time commitment for athletes and coaches is minimal.
Parents and players need to demand these programs and reduce the risk of the ACL injury downward spiral that plagues far too many athletes.
Does your team incorporate neuromuscular training programs? If not, does this information make you more eager to encourage starting a knee injury reduction program? Would the presence of absence of the training program influence selection of a particular team?