
Filtering by Tag: dance medicine
Dr. Koutures Publishes on Dancers and Concussion in Journal of Physical Education, Recreation and Dance

Dancers are “artistic athletes.” They must possess the strength, agility, power and flexibility of any athlete and perform with perfect musicality and emotion, demonstrating the artistry of the dance. As an art form dance continues to push the physical boundaries of the human body, increasing the inherent risks to the dancers. Most injuries are readily acknowledged as a possible outcome of being a performing artist; however, the possibility of a concussion continues to receive little attention by leaders involved in dance education. The majority of dance and physical education instructors continue to be oblivious to the prevalence, diagnostic procedures, symptoms and appropriate reintegration into the dance environment after a concussion. Adapting the existing knowledge regarding concussion and sports, this article provides fundamental information to support the recovery and return to performance of a dancer with a concussion.
Click here to read the remainder of this important article to learn about:
- Evaluation of concussion symptoms and severity
- Treatment protocols for dancers
- Dancer reintegration after concussion
Three Key Questions that can Reduce Overuse Injuries in Young Dancers
1. Am I going through a growth spurt?
Bottom Line: Longer arms and legs are harder to control without appropriate strength in the shoulder and hip areas. While many pre-teen and teenage dancers want to amp up dance commitments, growth periods are not the best time for adding more technically demanding routines. Stick to basic movements, build central strength, and once in better control, then more ready to step up the skill requirements.
2. Am I still getting over a past injury?
Bottom Line: Trying to push through a past injury that hasn't fully healed is a recipe for future trouble. Better to take a step back, get proper medical care, and when more healthy, then push ahead with more classes and more intense routines.
3. How old am I?
Bottom Line: Absolutely the best evidence out there to reduce overuse injuries, and very easy to remember. If your age in years is lower than the number of hours of organized dance activities per week, your injury risk goes up in dramatic fashion.
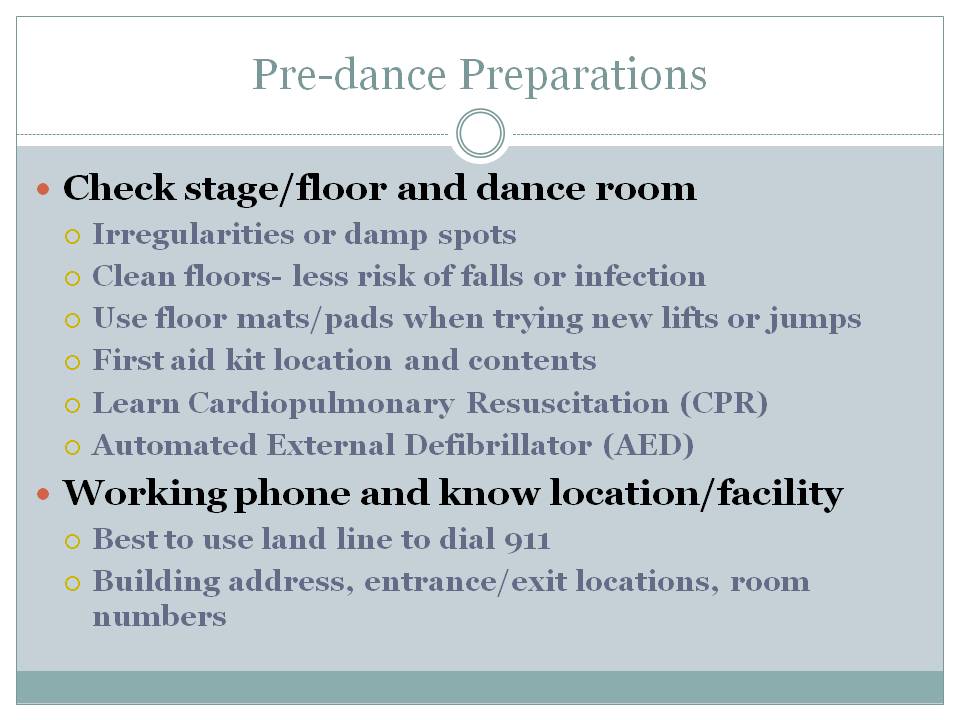
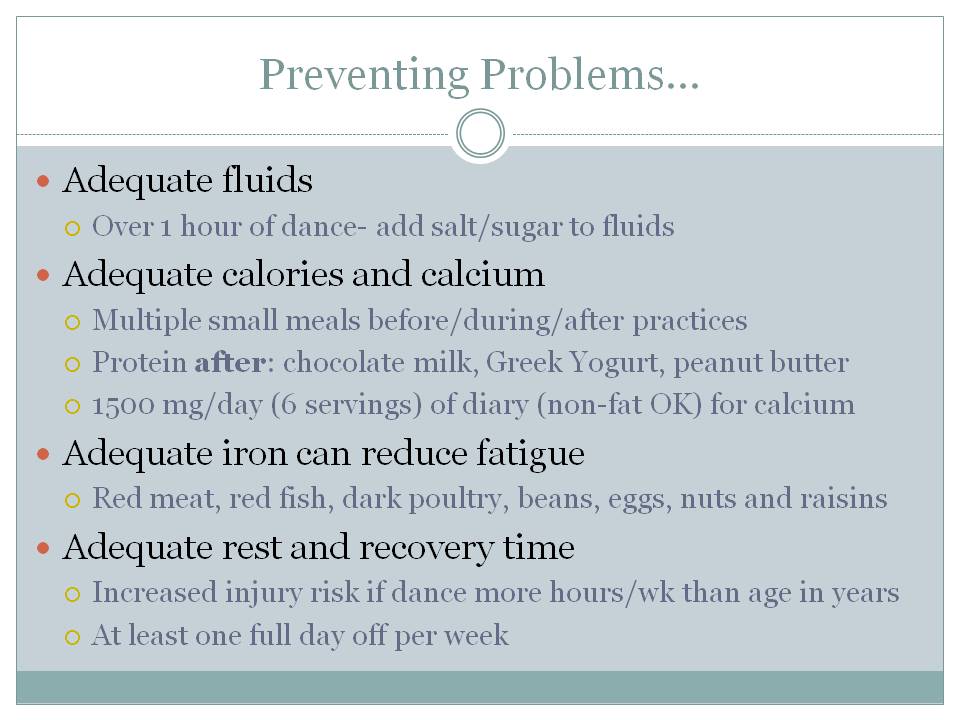
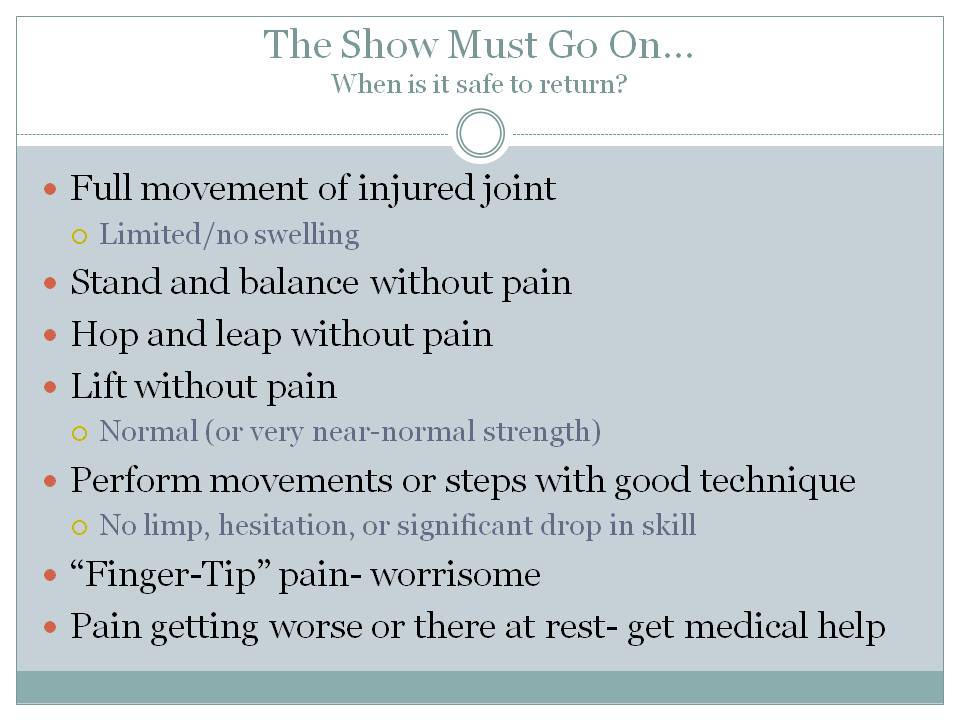
How to Prevent and Minimize Dance Injuries
Click on each slide to advance
Injury Prevention Tips for Adolescent Dancers
The following Injury Prevention Guidelines summarize findings from the article The Adolescent Dancer: Common Medical Conditions and Relevant Anticipatory Guidance by Kathleen Linzmeier, MD and Dr. Koutures which is published in Adolescent Medicine State of the Art Reviews, April 2015 and is copyright from the American Academy of Pediatrics.

1) The American Academy of Pediatrics recommends a rest period from organized physical activity that includes a minimum of 1 full day off per week and 2 to 3 months off per year.
3) Single sport or activity specialization at young ages can increase the risk of physical and emotional overuse, frequently leading to burnout and complete cessation of activity. Particular warning signs may include decreased interest in dance activities, lower school grades and attendance, less social interaction, changes in appetite or sleep, and mood alterations such as irritability, anger, or lack of fun or new activities.
4) Incorporating recommended weekly and annual rest intervals along with varying the types of organized activities can reduce the potential for burnout.
5) Medical practitioners may be asked for their opinion on the readiness of young dancers to begin dancing en pointe, which is an advanced ballet skill that places extreme stress on the lower leg, ankle, and foot
6) Readiness recommendations focus not on chronologic age but on the presence of adequate whole body strength and balance (especially of the foot and ankle), lack of current restricting injuries, sufficient “pre-pointe” dance class exposure (minimum 3-4 years), and the future goals of the dancer.
7) Medical professionals should maintain an open dialogue about adequate intake of calories and essential vitamins and minerals, and maintenance of healthy weight to best support ongoing dance activities.
8) Physicians should respect the anatomic and emotional changes that occur during puberty without hesitating to modify or change focus to more basic skills to allow compensation for changes in movement patterns and coordination.
An Intensive Effort to Reduce and Prevent Dance Injuries
Always a leader in cutting edge dance, Backhaus Dance is also front and center with promoting health dancer practices. Proud to be part of their Summer 2016 Intensive faculty and proud to share tips below with all dancers and dance educators.

Click on each slide to advance.
Dr. Koutures New Video Presentation Page
Check out new webpage with Video Presentations:
https://chris-koutures.squarespace.com/dr-koutures-videos/
Current Video Presentations include:






More to come- suggestions for future Video Presentation ideas eagerly accepted for consideration.
Video: Dr. Koutures Grand Rounds on Performing Arts Medical Care
August 20, 2014 - Grand Rounds - CHOC Children's Hospital
Click Here for Video: The Performing Arts Athlete: Anticipatory Guidance & Evaluation
Chris Koutures, MD, FAAP
Pediatric and Sports Medicine Specialist
Anaheim Hills, CA
Medical Team Physician, Cal State Fullerton and USA National Volleyball Teams
Outcomes - At the conclusion of this presentation, the physician leaner will be able to:
1. Provide anticipatory guidance to young dancers and performers about nutrition, rest, risk of overuse, and other key injury/illness concerns.
2. Appreciate the various forms of dance and recognize certain movements and positions that can lead to both acute and overuse injuries.
Highlights: Unique Challenges of Adolescent Performing Artist
Thanks to the Chapman University College of Performing Arts and the Performing Arts Medicine Association for hosting the 4th annual Healthy Approaches to the Training of Performing Artists Conference last weekend. Presented on Unique Challenges of the Adolescent Performer and will highlight key points below:










Hear This- Musicians and Dancers need to Protect their Hearing!
Saw a few aspiring Marching Band members this week for pre-participation exams, which did include a discussion on hearing protection. Like many younger performers, they didn't seem too concerned about a problem that may not present until many years down the road. Like many young performers, they also may not know about one of my favorite bands Spinal Tap, and if I can actually make a Spinal Tap reference to illustrate the importance of protecting hearing in musicians, I definitely won't miss the opportunity.
Oh, and after appreciated the music levels in dance classes, it would be best if dancers heeded this information as well!
Noise induced hearing loss can occur after a brief exposure to louder sounds, can be reversed if occurs earlier in life, but with repeated exposure to louder sounds, permanent damage can occur.
Noise induced hearing loss is also completely, 100% preventable!
My parents owned and operated a company that made audiograms (machines that test hearing) for around 30 years, so I have always been partial to the concerns of hearing loss.
In the case of musicians, they are at particular risk of higher frequency range hearing loss that can affect conversations and other daily activities as illustrated by the audiogram below:

The red line (right ear) indicates a significant hearing loss at 4000HZ and the blue line (left ear) shows a loss, though not as dramatic, at the same frequency. the 4000 HZ level includes hearing of several vowels, consonants and especially those involving the letter "s".
Regular (at least annual if not more frequently) audiograms along with noise monitoring equipment in practice rooms and performance halls can help a musician monitor hearing and noise exposure.
Noise travel can be deflected or decreased by the following techniques:
- Use of sound barriers between musicians
- Use of plexiglass shields between musicians
- Risers to alter the level of musicians and keep instruments from being placed right next to the ear of a fellow musicians
- Use of sound baffles in instruments
- Attention to position in room of both individuals and groups of musicians
Personal hearing protection may not always be the most popular aesthetic selection, but can be extremely useful:
- Ear Plugs
- Rubber, Plastic, Urethane, Wax, Foam or Impregnated Cotton
- Off-the-shelf Fairly Effective
- Ear Muffs
- May give a more effective seal
The final piece of protective advice- one doesn't have to max volume every performance, or in the words of our Spinal Tap mates, you don't have to go to 11 every time!
After reading this, are you more apt to use hearing protection techniques? Do you have any other suggestions to protect your hearing?
Is My Daughter Ready for Pointe Work? A Dance Medicine Physician Perspective
The decision to initiate pre-pointe training is a sentinel event in the progression of a young dancer. Dancing en pointe which involves full-weight bearing on the toes, is fundamentally rigorous, can lead to a variety of lower body injuries, and signifies a high level of commitment to ballet that should not be taken lightly.
Relying on reaching a certain to start (ie: "we start pointe at age 11") is not sensible and supported by many dance medicine authorities. Rather, there is the concept of developmental age which takes into account dance experience, mechanics, strength, commitment, and nutrition/sleep for a more individualized assessment of readiness.
Many wonderful musculoskeletal screening recommendations have been made by respected authorities, and I will definitely reference them below and do use them in my clinical practice.
Before moving the focus on movement patterns, I like to take a step back with dancers and families to discuss fundamental concepts emphasizing sufficient sleep, dance-specific nutrition and balance of dance classes and adequate time off for recovery. If a young dancer is not ready to accept these key foundations for success, then I'm not certain she is ready for the rigors and "sacrifices" of point work. Jeff Russell has an amazing review of how psychosocial traits of dancers, nutrition and fatigue all can contribute to injury and I highly recommend the read.
- Dancers must accept the unique physical and mental demands of point work leading to a need for increased sleep (minimum 8-9 hours a night)
- Adequate calcium (1000-1500 mg/day) and iron (15 mg/day) needs can be best addressed by 4-6 servings of dairy foods and 3-4 servings of meat/protein per day
- Minimum of 1-2 days off a week from organized activities to enhance recovery
Returning to the discussion of musculoskeletal readiness, The International Association for Dance Medicine and Science (IADMS) proposes the following guidelines:
- Not before age 12.
- If the student is not anatomically sound (e.g., insufficient ankle and foot plantar flexion range of motion; poor lower extremity alignment), do not allow pointe work.
- If she is not truly pre-professional, discourage pointe training.
- If she has weak trunk and pelvic ("core") muscles or weak legs, delay pointe work (and consider implementing a strengthening program).
- If the student is hypermobile in the feet and ankles, delay pointe work (and consider implementing a strengthening program).
- If ballet classes are only once a week, discourage pointe training.
- If ballet classes are twice a week, and none of the above applies, begin in the fourth year of training.
Prospective point dancers can benefit from a focused musculoskeletal screening examination, and the great team at Childrens Hospital of Kings Daughters has a nice visual which illustrates some of the following:
- Measuring range of motion of the ankle, foot and especially the great toe.
- Limitations in great toe range of motion can lead to injuries not only in the foot, but at the ankle and knee
- The Pencil Test can measure foot plantarflexion
- Loose tissues on the outside of the ankle, often from past ankle sprains, may not be able to handle the stresses of pointe leading to fractures of the talus (lower ankle bone) or 5th metatarsal bone on the outside of the foot
- Assessing strength and endurance of the "proximal" structures (hip, buttock, quadricep and hamstring muscles) where weakness leads to abnormal stresses on the inside of the knee, shin, and foot/ankle
- The Airplane Test has been associated with readiness for pointe work
- Single leg squat alignment, where hips, kneecaps, and 2nd toe should all stay in line, is a great measure of that proximal strength
- Collapse of the knee inward, excessive internal rotation of the shin, or significant collapse of the arch/rolling in of the foot are problem findings that should be addressed before starting pointe.
- I also like to put dancers perform plie in 2nd position- ideally inside of knee should be lined up over 2nd toe with minimal rolling in of foot.
- Inability to maintain this alignment is another problem area that should be addressed before starting pointe.
- If there is any history of past injury, the dancer should have completed a full rehabilitation program culminating in unrestricted return to dance before contemplating pointe work.
- The biggest risk to future injury is under-rehabilitated or lingering past injury
In any type of injury prevention and readiness assessment, communication is the name of the game. The results of a thoughtful medical and musculoskeletal assessment from a dance medicine specialist can be discussed with instructors and this collaboration is a wonderful medium to best prepare a young dancer when she is ready for pointe work.