Stress Injuries to the Tibia: A Video Interview
Sincere thanks to Matt Swift, DPT from Change Sports Physical Therapy Institute for creating this video on Stress Injuries to the Tibia with focus on symptoms, treatment, and prevention.

Please Check Our New Brand and Website: www.ActiveKidMD.com
Comprehensive blend of general pediatric and sport medicine care with an individualized approach that enhances the health and knowledge of patients and their families
ACCEPTING NEW PATIENTS- CALL 714-974-2220 FOR AN APPOINTMENT
CLICK HERE FOR DR. KOUTURES GENERAL PEDIATRICS INFORMATION
Proud physician:
USA Volleyball Mens/Womens National Teams
CS Fullerton Intercollegiate Athletics
Chapman University Dance Department
Orange Lutheran High School
Co-Author of Acclaimed Textbook
Pediatric Sports Medicine: Essentials for Office Evaluation
Orange County Physician Of Excellence, 2015 and 2016
Sincere thanks to Matt Swift, DPT from Change Sports Physical Therapy Institute for creating this video on Stress Injuries to the Tibia with focus on symptoms, treatment, and prevention.
Is it OK to exercise when sick? What symptoms should keep someone off the playing field?
When trying to decide if an athlete is too ill to participate in sports, I tend to ask the following questions:
Study and experience tells us that a fever over 100.4 degrees Fahrenheit may increase metabolic demands of the body, often making exercise more difficult. Thus, many authorities recommend starting with lighter levels of exercise with a fever, and using overall performance to advancing to higher intensity of exercise. Some athletes may perform quite adequately with a fever, while others will need complete rest from exercise until the fever is gone for at least 24 hours.
I have found that the neck rule can also assist athletes and parents in deciding on sport participation, with or without a fever:
How can we limit spread of colds and other illnesses during the winter months?
Multiple factors contribute to healthy function of the immune system in preventing illness
No athlete wants to be sick during the season and no athlete wants to spread illness to other team members. Following some basic rules can help prevent the spread of infections:
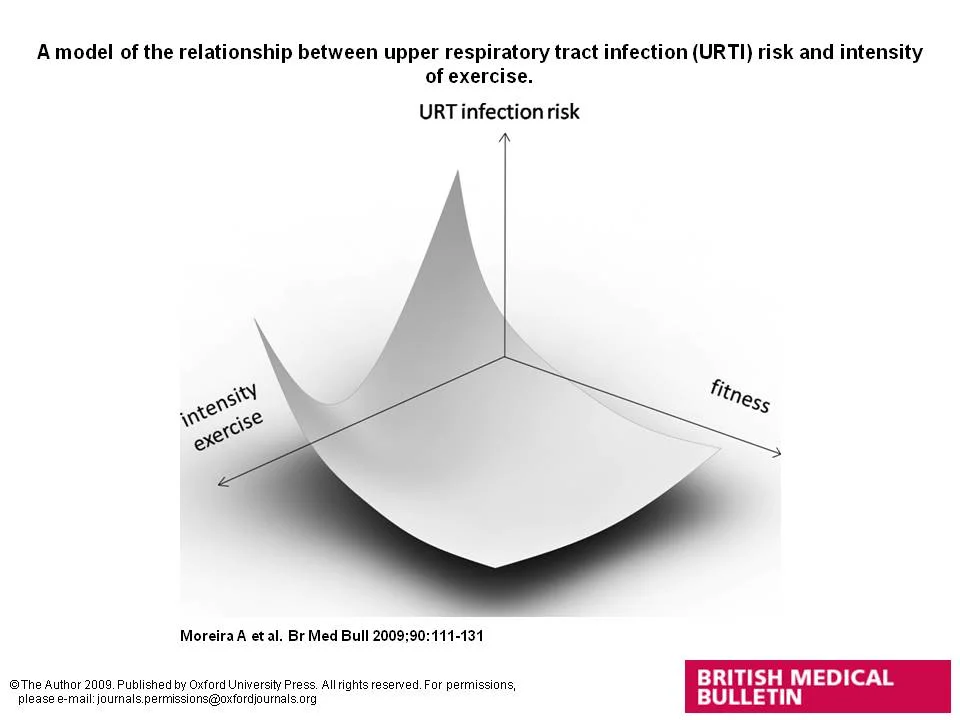
How does the amount of exercise influence risk of getting sick?
Moreira A et al. Br Med Bull 2009;90:111-131, © The Author 2009. Published by Oxford University Press. All rights reserved. For permissions, please e-mail: journals.permissions@oxfordjournals.org
The above figure demonstrates that both intensity of exercise and fitness level can influence the risk of upper respiratory infection. More moderate levels of exercise can be protective against illness, while lower levels and higher levels of exercise may actually be related to an increased risk. This is often why athletes get sick right after higher level competitions or at the end of a particular sport season. Higher levels of fitness may also be protective against respiratory illnesses.
There is no magic age at which a child can begin weight training. Readiness for weight training depends on the willingness of the child to lift weights, follow directions, and maintain the program for several months to see results. Remember, this is for the child, not for an adult or coach.
Weight training should supplement regular sport activity. It is not acceptable to have weight training injuries keep an athlete away from his/her sport. I recommend qualified supervision by a performance or physical trainer who routinely works with children and adolescents. The focus should be on appropriate-sized equipment, meticulous weight lifting technique, starting with low weights/high repetitions, and working multiple body parts. In appropriate program, a child will often lift weights 2 or 3 days a week with at least 48 hours of rest between sessions.
The physical results, such as muscle enlargement and weight gain, depend on the gender and developmental stage of the child. Routine weight training can make a child somewhat stronger by increasing nerve and muscle communication. However, if the child is looking for larger and more bulked muscles, then they must wait until after their growth spurt. Androgens are a particular hormone, produced more in boys than girls, which produce muscle and strength gains. Since androgens increase late in puberty right after the growth spurt (age 11-12 in girls, age 13-14 in boys) lifting before this time will not result in massive muscle bulking or extreme strength gains.
Does this mean one should not lift before the growth spurt? No, but just place the emphasis on good technique and reduce the expectations for big-time muscle gain. Remember, due to lower androgen production than boys, girls will have less increase in muscle mass.
Is weight training safe for children?
Studies have shown that a properly designed and supervised resistance training program can be safe for children and young adults. Contrary to popular belief, weight training at a young age does not stunt growth as long as proper techniques are utilized. There are reports of overuse injuries with back strains the most common but at no greater frequency than what is seen on the athletic field. Again, placing the emphasis on a properly designed and supervised resistance training program will help reduce injuries and maximize enjoyment.
Click here to learn about:Proper post-lifting recovery, focusing on nutrition and sleep, can greatly enhance the results and safety of a weight training program.
Does weight training work?
Both published studies and personal experience have shown impressive strength, speed, and endurance gains with an appropriate weight training program. There is no good scientific data to show that this directly translates to better on-field performance, but it does contribute to overall athletic ability. The athlete needs to be aware that he/she must stay with the program or risk losing the gains.
To produce optimal results, recommend starting a program during break periods between sport seasons and not initially scheduling weight training sessions on same days as practices or games. Once the athlete is more comfortable with the demands of weight training, can incorporate lifting sessions with regular training and competition activities.
Can weight training reduce injuries?
High school-based studies indicate a resistance training program could decrease the number and severity of injuries, and also reduce the rehabilitation time once an injury has occurred. These benefits may be due to stronger supporting joint structures, muscle absorbing more energy before tiring out, and greater muscle balance around a specific joint.
Can weight training help with weight loss or weight control in children?
Weight training programs that feature higher repetitions, lower weights and limited rest between sets have been shown to contribute to both weight loss and weight control in children. Appropriate professional supervision in designing such a program can be of significant help.
Thanks to colleagues at Intecore Physical Therapy for filming this video on Youth Arm Injury Prevention that has been distributed and shared with several local Little League groups.
I have accessed CoachSmart while on the sidelines, and no longer have to guess or try to remember suggested adjustments for practice and games in hot or humid weather. The information is concisely presented in the palm of my hand.
The iPhone app CoachSmart was developed by colleagues at Vanderbilt Sports Medicine and the Monroe Carell Jr. Children’s Hospital at Vanderbilt and is billed as the ultimate resource for coaches, offering real-time information on heat index and lightning strikes, frequently asked sports medicine and safety questions, and a group contact feature.
The The app is free to download in iTunes with an annual in-app subscription to live lightning data for $1.99.
Developed by Sports Medicine Physicians and Athletic Trainers with close guidance from coaches, the CoachSmart app brings many important topics into one easy location.
Recommending CoachSmart is now part of my pre-season safety talks to coaches, parents, and administrators, and will also be part of an upcoming lecture on Heat Illness.
The CoachSmart App was recently upgraded and returned to active status. I do not have any financial relationship with the CoachSmart App.
To read my post, please click here
For years, I have heard claims that some Major League Teams favor drafting pitchers who grew up in colder climates.
The reason?
Fewer months able to be spent outside likely means fewer competitive pitches thrown, fewer innings pitched, and perhaps less risk of cumulative stress to shoulders and elbows. Practicing pediatric sports medicine in almost too sunny Southern California (yes indeed, we desperately need rain) I commonly encounter young throwers who pitch most if not almost all months of the year.
Now, thanks to the recent study Is Tommy John Surgery Performed More Frequently in Major League Baseball Pitchers From Warm Weather Areas?, there might actually be some scientific confirmation to these concerns.
Based on rates of elbow medial ulnar collateral ligament (UCL) reconstruction (commonly known as Tommy John Surgery) in Major League pitchers who played high school baseball in warmer vs. colder climates (defined by latitude on map and mean average temperatures), those who grew up in the warmth were found to have a more frequent and earlier UCL reconstructions than players who grew up in the colder environments.
I also found another interesting finding that almost 2/3 of the Major League pitchers in the study pool from 1974 to June 1, 2014 were from colder climates, while by the definitions utilized of warmer vs. colder climates, almost 2/3 of the 73 total studied areas were in colder climates while only 23 of 73 areas were defined as warmer. This correlation does make sense from a general statistical model, but when considering that the warmer areas contain purported baseball hotbeds such as California, Florida, Texas and countries in the Caribbean, Central and South America, the 2/3 proportion coming from colder climates again might support the higher risk cumulative stress and injury in warmer, more possible year-round baseball climates. Perhaps hibernating from too much pitching is ultimately a protective and positive thing and not just another reason to complain about bad weather in certain regions.
The published results on Major League pitchers should not be directly correlated with injury risk to pitchers at the pre-high school, high school and even collegiate or minor league levels. However, if similar studies were conducted at those levels with comparison of UCL reconstruction rates between climates, I wouldn't be too surprised if the surgical frequencies were higher in warmer climates and possibly starting at younger ages as well.
The upshot of this post is not an endorsement or call for relocation to colder climates to foster a potential Major League Pitching career, but rather a cautionary tale that even in those fortunate and talented enough to pitch in the Major Leagues, the potential blessings to have year-round chances to competitively pitch must be tempered with the need for adequate rest and recovery. I think this need to not take undue advantage of virtually unlimited pitching opportunities does definitely correlate down to school-age and collegiate/minor league pitchers.
Once again, we are getting the message that more is not often better, especially in the long-term development of young athletes.
I've had the pleasure of coaching my young twin sons in baseball over the past two seasons, and like many coaches I constantly wonder about how well I am doing with teaching the basics and strategies of this great sport.
Put me in my pediatric sports medicine specialist role, and once again, I am constantly wondering about how well we in the injury prevention community are doing with teaching the basics of injury prevention and translating our knowledge to fellow coaches, parents, and ultimately, to our players.
Let's take the case of arm injuries in young pitchers as an example.
After the realization that too much throwing over the course of a single season and through an entire year both increase the risk of elbow and shoulder injuries in young pitchers, well-researched Pitch Count Recommendations in Young Pitchers were developed and promoted by many sports medicine groups and youth baseball organizations. These guidelines included not allowing young pitchers to throw with any aspect of shoulder or elbow pain.
So, with these great recommendations discussed in lecture halls, outlined on websites, and passed out on brochures and handouts, how are they actually playing out on the diamonds?
Based on the results of two recent studies, those efforts appear to be mostly striking out.
Allison Gilmore, MD and colleagues from Case Western University in Cleveland, OH presented some unique findings from a recent study indicating that pitch count recommendations are not routinely utilized by Little League coaches or parents.
Less than 10% of coaches regularly monitored and set safe limits for amount of pitching over the course of a year, and 41% reported having players who were at-risk for arm injuries due to playing on more than one baseball team during a particular season. These findings probably fall at least equally on the shoulders of parents who allow the year-round or multiple team participation.
The apparent acute impact of this lack of compliance? More than 1/3 of coaches had a player unable to play due to an overuse injury.
These results echo those of 2012 study on Knowledge and Compliance With Pitch Count Recommendations: A Survey of Youth Baseball Coaches which had 228 Little League (age 9-15) coaches complete an 18 question survey testing knowledge of pitch count recommendations that indicated:
Significant conclusions included concerns over difficulties of coaches following unfamiliar recommendations and potential of greater enforcement efforts by leagues.
As I mull over the findings of these studies, I struggle with the apparent gap between policy and practice and how to best bridge the gap.
Perhaps we in the sports medicine field are the victims of outstanding results of our surgical and rehabilitative efforts? The growing list of pitchers returning to star on the field after potentially career-threatening arm injuries may give an elevated or almost false hope that injury prevention is less important because amazing treatment results are readily available.
Perhaps its because as parents and coaches we still hang on to the adolescent vibe of invincibility- that nothing bad will happen to our kids.
Perhaps the teachers haven't found out the optimal ways to best reach and teach. Is it social media, videos, 1:1 tutorials, high profile pleas?
For now, the wondering will go on.
It can be an awesome feeling to be "in the zone" or "performing better than I have in years”.
It however, can be a major downer when that peak performance comes at a cost to immediate health and the immune system.
Anyone who has been around the time of a big show knows how performers like to celebrate afterward. That's right- everyone tends to get sick.
Exchange the big show for the big race or big competition and you often see the same outcome- many athletes go from the podium or finish line to the sick bed. Saw it at the Olympics where my first up close and personal views of gold, silver and bronze medals were around the necks of athletes coming in to the medical unit for upper respiratory infection evaluations.
Those were the fortunate ones who had timed their peak performance to occur at the Games and didn't have unplanned illness interrupt training or competition.
Unfortunately, many times this fairly tale ending doesn't occur. Peak performance earlier in a season leads to mid-season illness and eventual disappointment. Solid evidence tells us that moderate levels of physical exertion are protective against illness, while higher extremes of activity can diminish immune defenses and increase illness risk. Having a solid base of fitness before assuming more rigorous training can also reduce risk of diminished immunity and increased chance of illness.
It is nearly impossible to maintain peak performance for too long, especially over a schedule of multiple events combined with the stressors of school, homework, and a social life.
Trying to get adequate sleep (minimum 8 hours a night), proper nutrition including berries, cherries, and fish for the anti-inflammatory effect, and planned off days from training and competition can help combat the stressors that sap performance.
More important is adhering to the principles of periodization, where well-constructed training blocks are created to allow peaking at optimal times while also maintaining periods of relative rest and recovery.
So, if an athlete tells me "I'm at my best" right before a chosen high level competition, then less cause for concern. Still might get sick afterward, but the merging of preparation and schedule hopefully is fairly favorable.
If an athlete is peaking well before that big competition which is still weeks or months away or with many of my young athletes when they have to get up every week because "every game is a big game", then my worry starts to go up.
Nothing worse than showing up in the doctor's office missing key training days or even worse, important competition time due to illness. Enhancing the immune system with proper rest and recovery can lead to more visits in the winner's circle and less time scheduling visits with the medical staff.
Not that I can't handle bravado or a bit of embellishment.
I am genuinely excited to share the accomplishments of many of my young patients, but also do get worried about what the "gifted label" means for the athlete and just as importantly, for those around him or her.
Human nature tends to draw us closer to those who are physically gifted- we admire their talents, rarely tire of seeing them perform such wonderful feats, and often want them to be on the best teams and in the star positions. It can be a the stuff that is seen in dreams: to be asked to play "up with the older kids", frequently get asked to play on multiple teams, and often get the ball in crunch time.
However, this seemingly gratifying situation can quickly lead to bad dreams when we also realize that overburdening our most talented young athletes can possibly deter if not destroy their future sport and exercise ambitions. In his moving piece Are We Destroying Our Biggest Talents?, prominent sports research scientist Roald Bahr laments the consequences of such overload and quite eloquently advocates for extra caution in managing expectations and workload for our most gifted athletes.
Dr. Bahr's work centers mostly around repetitive jumping and hitting in volleyball (a shared passion) but also cites examples of frequent throwing in baseball and cricket as additional evidence of the propensity of excessive overload in star young athletes.
The development of pitch counts in baseball is but one effort to objectively measure and hopefully limit cumulative overload, and similar possibilities including jump counts and monitoring the number of hours per week in sport activity are sensible avenues to consider. Sufficient rest, attention to proper nutrition, and adhering to the principles of periodization which include coordinated, individualized, progressive changes in training intensity, frequency and volume are all necessary components of a comprehensive sport program for all young athletes, particularly those perceived to have the most talent.
I also will bring to your attention a summary of the seminal work of Carol Dweck, a prominent psychologist who developed a comparison between the fixed mindset and the growth mindset. All credit for graphic below to Ray Lokar from the Positive Coaching Alliance.
Many have seen gifted young athletes perceive their talents to be innate and developed from birth leading to diminished effort, avoiding of challenges, a fear of failure, and eventual early plateau. Combing early success with a growth mentality that embraces challenge and growth, even through failure, may lead to unprecedented levels of future success.
Check out a great review of the Fixed vs. Growth Mindset by the Huffington Post (courtesy of Positive Coaching Alliance).
So if you are one of the best or a parent/coach/instructor of one of the best our there, I offer both my sincere admiration and professional reminders about certain responsibilities:
My best wishes to keep young athletes playing at their best!
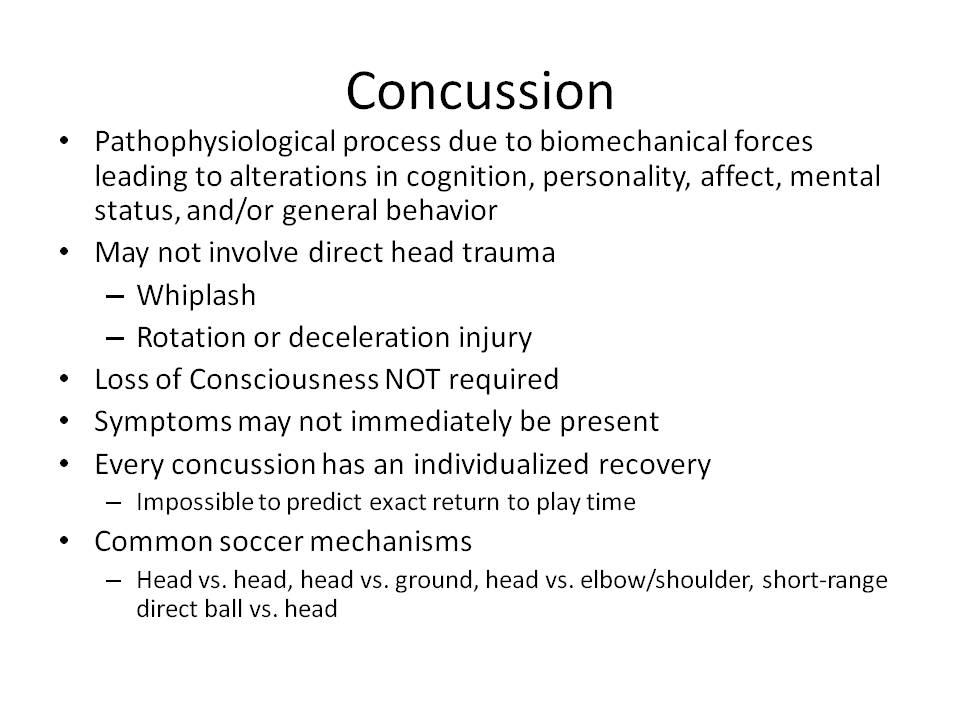
My wonderful colleagues at Concussion Connection have been offering their expert perspectives on retirement from sport due to concussion, and I am pleased to offer thoughts on the Social Impact of Retiring. Strongly recommend checking out the entire Concussion Connection site and praise them for the fine work they do in advocacy and education.
August 20, 2014 - Grand Rounds - CHOC Children's Hospital
Chris Koutures, MD, FAAP
Pediatric and Sports Medicine Specialist
Anaheim Hills, CA
Medical Team Physician, Cal State Fullerton and USA National Volleyball Teams
Outcomes - At the conclusion of this presentation, the physician leaner will be able to:
1. Provide anticipatory guidance to young dancers and performers about nutrition, rest, risk of overuse, and other key injury/illness concerns.
2. Appreciate the various forms of dance and recognize certain movements and positions that can lead to both acute and overuse injuries.
Are you a well-meaning coach trying to get the most out of your athletes during early morning training sessions? Somewhat frustrated that everyone seems a step slow or out of sorts during zero period? While "morning people" are a dime a dozen in the adult world, doesn't it seem that finding teenagers raring to go at 0600 is like the proverbial needle in a haystack?
According to a timely American Academy of Pediatrics (AAP) policy statement on School Start Times for Adolescents this type of behavior is not just an irritating by-product of teenage rebellion and striving for independence, but is a consequence of age-related delays in release of melatonin (hormone that influences sleep onset) and a slower drive to fall asleep compared with non-adolescents.
So yes, teenagers are biologically designed to have their own (circadian) rhythms and if they truly ran the world (instead of thinking that they do) they would select later school start times around the order of 8:30 if not later. This does often conflict with the usual norms of the adult-oriented world (such as parents having to be at work by 9 AM) and the realities of limited access to pools and court space along with trying to fit in another activity into already tight class schedules.
The ultimate goal according to the AAP and its review of the scientific literature would be to provide a consistent 8.5-9.5 hours of sleep per night and reduce the consequences of cumulative sleep deprivation:
How do we best respond to these sleep deprivation concerns?
First of all, don't think that teenagers shouldn't get off without taking some responsibility for their less than impressive sleep statistics, as they often do not do themselves any favors with poor sleep initiation behaviors such as late night caffeine use, using electronics and media right before bedtime, and having access to television in bedrooms. Modifying some of these habits definitely could should be a high priority for parents, coaches, and educators with emphasis on the importance of sleep in post-activity recovery, preparation for next day activity, and especially the impact of insufficient sleep in mood and academic focus:
While giving appropriate counsel to sleep hygiene behaviors, there are certain nutritional recommendations that may also increase the quality of sleep initiation and maintenance according to an article conveniently published just before the AAP article:
Finally, those of schedule-making adults might want to take a hard and scientific look at the utility of early-morning activities designed for adolescents. While the decision for later school starts may not be part of your pay grade, carefully weighing the risks and benefits of zero period weight training sessions or other before school activities in favor of more after school activities may actually increase athletic and academic performance in this age group. Delaying the start of afternoon training or competition sessions to allow for that brief nap (again, under an hour) may also enhance overall performance and mood of the team or group.
Do these sound like sensible and realistic recommendations to address sleep issues in adolescents?
Below is a copy of the slide presentation:
Greatly appreciate the opportunity to share thoughts with Lindsay Barton, who tackled the hot topic of Heading in Youth Soccer for MomsTeam.com with a very well researched and balanced article released this week.
Barton referenced the American Academy of Pediatrics Council on Sports Medicine and Fitness policy statement regarding Injuries in Youth Soccer that I helped co-author, and also reviewed many recent studies and other policy statements on the subject.
Strongly recommend that anyone interested in the health and development of young soccer players take the time to read Barton's piece.
Saw a few aspiring Marching Band members this week for pre-participation exams, which did include a discussion on hearing protection. Like many younger performers, they didn't seem too concerned about a problem that may not present until many years down the road. Like many young performers, they also may not know about one of my favorite bands Spinal Tap, and if I can actually make a Spinal Tap reference to illustrate the importance of protecting hearing in musicians, I definitely won't miss the opportunity.
Oh, and after appreciated the music levels in dance classes, it would be best if dancers heeded this information as well!
Noise induced hearing loss can occur after a brief exposure to louder sounds, can be reversed if occurs earlier in life, but with repeated exposure to louder sounds, permanent damage can occur.
Noise induced hearing loss is also completely, 100% preventable!
My parents owned and operated a company that made audiograms (machines that test hearing) for around 30 years, so I have always been partial to the concerns of hearing loss.
In the case of musicians, they are at particular risk of higher frequency range hearing loss that can affect conversations and other daily activities as illustrated by the audiogram below:
The red line (right ear) indicates a significant hearing loss at 4000HZ and the blue line (left ear) shows a loss, though not as dramatic, at the same frequency. the 4000 HZ level includes hearing of several vowels, consonants and especially those involving the letter "s".
Regular (at least annual if not more frequently) audiograms along with noise monitoring equipment in practice rooms and performance halls can help a musician monitor hearing and noise exposure.
Noise travel can be deflected or decreased by the following techniques:
Personal hearing protection may not always be the most popular aesthetic selection, but can be extremely useful:
The final piece of protective advice- one doesn't have to max volume every performance, or in the words of our Spinal Tap mates, you don't have to go to 11 every time!
After reading this, are you more apt to use hearing protection techniques? Do you have any other suggestions to protect your hearing?
Ankle sprains are the most common acute injury in indoor volleyball, and very few things spark intense debate in the volleyball community more than the question about using ankle braces to prevent these type of injuries.
Photo courtesy of USAVolleyball
I'm going to review this subject by not only listing some studies about ankle braces, but more importantly tapping the awesome collective wisdom of my USA Volleyball Sports Medicine colleagues Aaron Brock, ATC and Jill Wosmek, ATC who work with Men's and Women's National Teams respectively. I am not going to review ankle taping, since many athletes do not have access to proper ankle tape applications by athletic trainers, and even when done well, tape looses most of the protective effect within 30 minutes of application.
The majority of ankle sprains are when the ankle inverts (rolls in) and this most often occurs with play at the net where athletes make contact with another players foot when landing from a jump during hitting or blocking. The theory behind bracing is to reduce abnormal ankle motion, but some fear that depending on bracing might make lower leg supporting muscles weaker and maybe even increase the risk of knee injuries.
I do not endorse or have any investment in particular types of braces, and will only list particular brands and makers if they were mentioned in studies and all opinions are our own and do not represent official policy of USA Volleyball or any other group or employer.
What does the medical literature say about this?
What do my expert volleyball medicine colleagues have to add?
In his experience working as the Director of Sports Medicine and Performance and the Head Men's Athletic Trainer for USA Volleyball, Aaron Brock has the following insight:
As the Head Athletic Trainer for the USA Women's National Team and formerly the athletic trainer for Penn State Men's and Women's Volleyball Teams, Jill Wosmek offers her professional recommendations:
Does this information make you more or less apt to use ankle bracing and strengthening programs to reduce the risk of ankle sprains?
Watch this Video on How to Prevent the Six Most Common Volleyball Injuries
Sudden Cardiac Collapse (SCC) can occur almost anywhere, and far too often, it takes place at athletic events and facilities. Our local community was painfully reminded of this a few weeks ago with the tragic collapse and ultimate death of a high school student.
Once someone collapses, immediate initiation of Cardiopulmonary Resuscitation (CPR) and use of an Automated Electronic Defibrillator (AED) are the only ways to prevent death and time is indeed of the essence:
So before participation in any athletic activity, parents and athletes need to ask 2 key questions:
Knowing how to perform CPR should be standard training for all coaches, officials, administrators, parents, and yes, even athletes. Good studies have shown that kids as young as 5th grade can appropriately perform these lifesaving skills. Low cost classes are available in almost all communities that take only a few hours to learn/review the elements of CPR and AED use.
Learning how to use an AED is rendered meaningless if there isn't an AED unit available on site in the event of a sudden collapse. While AED placement is now commonly seen at shopping malls, churches, on airplanes, and in large workplaces, it is defeating to learn how often school or athletic facilities do not have a unit in public view and available for immediate use.
Highly recommend that upon arriving at any field, gym, or exercise facility, look around or ask about the location and availability of an AED. Just like identifying the nearest exit in event of a fire or other emergency, knowing AED placement can reduce time needed to put it into use when those seconds definitely count. Proper pre-participation preparation and emergency action plans should involve informing as many people as possible about the location and use of the AED.
If there isn't an AED, don't be afraid to make a little noise by advocating for placement. In many cases, concerns about liability, cost, maintenance, and training have been overcome by passionate community efforts emphasizing the benefits of having an AED for the greater good of athletes and spectators alike.
My wife and I just completed our CPR and AED recertification this week (thanks to Heartsavers in Fullerton, CA for such a wonderful course) and hope to have all readers of this blog join us in learning these skills that can make such a difference.